
One beautiful day last December, an old friend and I were making Christmas puddings. At the time, I was working on a story – this story – about menopause, and because she’s one of the few people who’s ever mentioned the subject to me, I asked her about it. She paused in our endless chopping of dried fruit and rolled her eyes. “I talk about it, but nobody else does,” she said. “And I think perimenopause is even more what people don’t speak about, if that’s possible. I had no idea what was going on when it happened to me – literally no idea. Was I just really tired? And really hot, because it was summer? And why was I so angry – an almost out-of-body feeling of rage, totally out of proportion to the event? What was all that about?”
My friend has a university degree; she’s been a journalist for almost 20 years; she’s a performer with a famous feminist theatre group. And yet the entire process of menopause was a mystery to her when it began five years ago. “I know it sounds bizarre, but you only learn about it by some kind of osmosis,” she said. “Sometimes I get my period app out, and I’m like, ‘Hmm, 185 weeks late.’ So yes, I’m in menopause. But who knew?”
The North American Menopause Society calculates that by 2025, there will be 1.1 billion post-menopausal women. And in the past couple of years, as more Gen X women – according to Forbes magazine the “healthiest, wealthiest, and most active generation in history” – begin reaching menopause, a new “menopower” movement has taken shape. You can now buy a raft of books about menopause, listen to hundreds of podcasts, watch documentaries, attend menopause retreats, throw menopause parties and purchase endless fashionable products and potions, mostly unknown to science, all apparently capable of resolving any menopause problem. Celebrities like Gywneth Paltrow, Naomi Watts and Serena Williams are all investors in the global wellness menopause industry, which barely existed five years ago but is projected to be worth US$600 billion ($840 billion) by 2025.
“This is the start of a new [product] category, and everyone has jumped in, but I think we could be at risk of ‘menowashing.’ ”
An offshoot of the unimaginably vast beauty and wellbeing industries, this new menopause market is full of “vaginal wellness” formulations, skincare ranges, hair “densifying” treatments and a bewildering array of probiotics and vitamin supplements – so many that even experts are startled. “I am nervous about where this market is going,” admitted Millie Kendall, CEO of the British Beauty Council, last October. “This is the start of a new [product] category, and everyone has jumped in, but I think we could be at risk of ‘menowashing’ ” – rebranding existing ingredients (and raising their price tags) to cash in on menopause demand.
Loading
It’s not just a (somewhat ambivalent) consumer revolution, however. In November, the Australian Workers’ Union, the Transport Workers’ Union, the Rail, Tram and Bus Union and the United Workers Union announced they would campaign to have menstrual and menopause leave enshrined in the Fair Work Act; in the same month, in NSW the Perrottet government announced the launch of four menopause health hubs and 12 connected services to provide specialised menopause care.
In Victoria, meanwhile, the Andrews government made a November election promise to commit $71 million towards 20 women’s health clinics across the state to provide “wrap-around” support for a range of issues including menopause. And last October, the Australian Institute of Superannuation Trustees asked the federal government to investigate their estimate of at least $15.2 billion per year in lost earnings and superannuation by Australian women due to menopause. There’s even a Menopause Day, a third of the way through Menopause Month, on October 11.
Pouring Christmas pudding brandy into tumblers, I asked my friend where she was on Menopause Day. “What? Oh my god.” She laughed. “We have moustaches on buses for a whole month, but nobody knows Menopause Day even exists!”


Serena Williams and Gwyneth Paltrow have both invested in menopause-related start-ups. Williams called it an “obvious” choice.Credit:Getty Images
Medically speaking, menopause itself did not exist until the 1820s. In 1821, French physician Monsieur Charles de Gardanne coined the trendy new term to describe a cluster of disorders affecting women in their 40s and 50s, including “epilepsy, nymphomania, gout, hysterical fits and cancer”. Some 19th-century doctors also believed menopausal women grew scales on their breasts and suffered from “morbid irrationality”, “minor forms of hysteria”, “melancholia and the impulses to drink spirits, to steal, and perchance, to murder”. Understandable, perhaps, if the world believed you were morphing into a sex-crazed lizard woman.
Today, we do at least understand the basic biological process of menopause. Perimenopause – a term that, like so much else in the menopause world, has only come to wide attention in recent years – describes the final phase of a woman’s reproductive cycle, during which fluctuating hormones, most significantly oestrogen, cause many of menopause’s infamous “symptoms”, including hot flushes and night sweats (which affect 75 per cent of Australian women in some form); insomnia and irritability (as many as 60 per cent); body aches and soreness (some 58 per cent), vaginal and genito-urinary problems (about 50 per cent); heavy, irregular, weird-in-other-ways periods (up to 90 per cent, depending on age); low libido (approximately 12 per cent at mid-life) and 30-odd other symptoms, including everything from itchy skin to vision changes and something called, bizarrely, “burning mouth”.
Menopause itself, when finally reached, is only diagnosed retrospectively, and often inaccurately: it’s the point one year after a woman’s final period. She’s then post-menopausal for the rest of her life. The average age of women at menopause in Australia is 51; perimenopause lasts on average anywhere from four to 10 years. The symptoms associated with menopause may persist long after menopause itself; and the average Australian woman lives for 32 years after menopause.
“They’re stressed, they’re angry, they can’t sleep and they have low sex drive. Is that menopause, or is that life?”
Loading
Despite its startling collection of potentially long-lasting impacts, many women never seek medical help for menopause. Of course, for some women, it’s a genuinely low-key event. And for many others, “there’s a certain amount of shit women just put up with,” says Dr Annie Marshall, a GP in Sydney’s inner west who specialises in women’s health. “I often have to really tease out perimenopause symptoms. These are women who are mid-career, they have school-aged children, they have elderly parents, they have crippling mortgages, and they have husbands they’ve been with for decades. So they’re stressed, they’re angry, they can’t sleep and they have low sex drive. Is that menopause, or is that life?”
They’re also hampered by social stigma and taboos. “There’s more embarrassment, less knowledge and more dismissal attached to menopause than to any other transition in women’s lives,” says author Kaz Cooke, who should know: she’s written books about pregnancy, parenting and problem periods. (She’s now working on a book about menopause, due out in October.)
Actor Naomi Watts sought to fill the conversation gap by launching a line of humorous greeting cards. One declares: “Perimenopause! It’s like puberty, except nobody knows when it will start or end; we don’t talk about it; they don’t make cute menopause movies … Clearly, it’s up to us to celebrate surviving this shit, so I got you this card.” Another hails “the breathtaking power of truly not giving a shit what anyone thinks any more”.
Another challenge is the militant note struck by many celebrity campaigners, who insist that menopause and its effects are optional, and that women can (and, by implication, should) fight its effects – usually by buying the very miracle products the celebrities happen to be spruiking. “We are not interested in being middle-aged,” claimed US celebrity stylist Stacy London recently. London was the CEO of short-lived “femtech” company State of Menopause, and despite her company’s closure in December she remains keen on “amplifying all the voices in this space”. “We have Botox, we have fillers, we go to the gym, we walk 10,000 steps, we’re going to live to be 90,” she said. “So we are not making middle age a thing. We’re going to just extend our youth span.”


Author Kaz Cooke: “There’s less knowledge and more dismissal attached to menopause than to any other transition in women’s lives.”
“I’m not at all sure about that whole ‘menopause is freedom, you should be magnificent; you should look 28 and wear a lot of high heels’ thing,” responds Kaz Cooke. “But then, the opposite is just as bad” – the idea that because homo sapiens females live an unusually long time beyond their reproductive years, “old” women must have some survival value to the species. “I hate that argument,” says Cooke: “that even though you’re some post-menopausal old bag, you’re allowed to be alive because you’re useful looking after children or cleaning the cave or whatever. I’m bloody sick of women being told there’s only one way to be.”
Dr Ginni Mansberg is a Sydney-based GP with more than 30 years’ experience – she’s appeared on SBS and Channel 7, and hosted Foxtel’s Embarrassing Bodies Down Under, as well as appearing in the Very Peri Summit online, hosted last year by Mia Freedman (who, with her knack of divining the Australian female zeitgeist, has recently waded into the menopause mire). “I specialise in women’s health, but a few years ago I realised I knew nothing about menopause – less than nothing,” Mansberg recalls. “In fact, I was a bit dismissive of patients who came to see me about it: a bit of that ‘suck it up, princess’ mentality. That’s not unusual among doctors, but I feel terribly guilty about it now – really ashamed. Because the more I learnt, the more I realised how complex and grim it can be.” Today, about a third of Mansberg’s patients see her for menopause-related issues, and in 2020 she wrote a book, The M Word: How to Thrive in Menopause.
Loading
“We have some of the best menopause experts in the world in Australia, but also a lot of doctors who’ve never had any training or experience at all. And there’s a bit of an art to prescribing for it, so you’ve got to find someone with some expertise and interest. Otherwise it’s hopeless. It would be like me examining a penis. I’m happy to do it, but I’m not sure my conclusions would be all that valuable.”
Most medical schools today, all over the world, almost entirely ignore menopause. In Australia, only one university, Melbourne’s Monash, has a barrier test (meaning students must pass it) for menopause training; in a global study published in October last year, researchers concluded that “overall, training on menopause management is profoundly inadequate”. This is despite extremely good reasons for both health professionals and women to take menopause seriously.
“We have some of the best menopause experts in the world in Australia, but also a lot of doctors who’ve never had any training or experience at all.”
Susan Davis is head of the Monash University Women’s Health Research Program, a consultant endocrinologist and head of the Women’s Endocrine Clinic at Melbourne’s Alfred Hospital. She’s also an adviser to the NHS Menopause Improvement Programme Steering Committee in the UK. In 2019, she led a qualitative study to find out what Australian women knew about menopause. “What shocked me was the almost complete absence of knowledge about the potential long-term health effects of menopause,” she says. The fact is, “the loss of oestrogen during menopause can affect your osteoporosis risk, your blood pressure, your cholesterol, and your cardiovascular health. Very few women know anything about that.”
For this reason, says Davis, every woman should have a comprehensive health check to assess bone density, cardiac risk and cholesterol levels, within a year or two of actual menopause, “regardless of whether you’ve had any menopause symptoms or not. There are changes in your body at menopause that can influence your health for the rest of your life.”
Many women are never told about such health checks, and many doctors never perform them. And this is because the medical profession – with some honourable exceptions – has spent an entire generation pretending menopause doesn’t exist. And that’s thanks to a single study, and a single set of results, published in 2002.


Dr Ginni Mansberg, pictured with media entrepreneur Mia Freedman. “A few years ago,” says the GP, “I realised I knew nothing about menopause.”
July 10, 2002 was the worst day of John Eden’s life. That morning, as usual, he walked into the garden of his Sydney home to collect the paper for his wife. There on the front page, in blaring tabloid headlines, were the words: “Stop your HRT and see your doctor!” “My god,” Eden recalls. “It was such a shock. Completely catastrophic language – and completely incorrect.”
HRT – hormone replacement therapy – was, and is, the treatment of menopause using oestrogen and, usually, progestogen, to replace the body’s own supplies. Starting from the 1940s, HRT became the magic elixir of menopausal life. But in 2002, an enormous US study of more than 160,000 women, called the Women’s Health Initiative, seemed to have discovered that HRT was a killer. It apparently caused increased risk of heart disease (29 per cent), strokes (41 per cent) and – the real shocker – a 26 per cent increased risk of breast cancer.
“Ninety-five per cent of my women went off their HRT immediately,” recalls Eden, who is associate professor of reproductive endocrinology at the University of NSW, director of the Sydney Menopause Centre at Sydney’s Royal Hospital for Women, and a founding director of the Women’s Health and Research Institute of Australia. “Somewhere between 300,000 and 400,000 women in Australia stopped taking it – some with severe menopause symptoms: five to 10 hot flushes an hour, waking every half-hour at night. They were devastated. The whole thing was appalling.”
Rod Baber agrees. Today he’s head of the menopause and menstrual disorders clinic at Sydney’s Royal North Shore Hospital, a past president of the International Menopause Society, and current editor-in-chief of the definitive international menopause journal Climacteric. But even he was unable to hold back the flood of women binning their HRT. “I remember a patient who was a GP; I had delivered her children. She rang me up and said, ‘You betrayed us.’ That’s how emotive it was.”
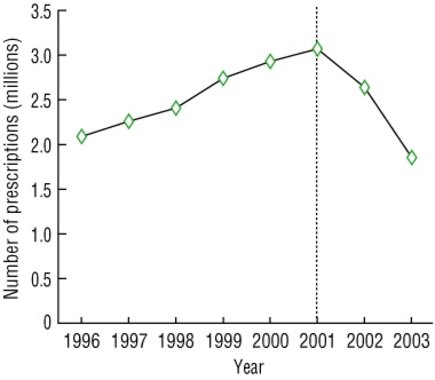
Hormone replacement therapy (HRT) prescriptions among concession cardholders in Australia, 1996–2003. In 2002, a US study triggered global headlines suggesting that HRT was a killer.Credit:Medical Journal of Australia
What made it even more painful was that the headlines were wrong. The women in the study were far older than many of the women in their 40s and 50s taking HRT in the real world, so their responses to it were different (today, it’s understood that women should begin hormone therapy before 60, or within 10 years of actual menopause). The study’s women were also significantly older than the placebo group they were measured against, which meant the results were skewed: the incidence of cancer and heart disease naturally increases with age.
Today, the Australasian Menopause Society and other international peak bodies agree that for healthy women without risk factors, starting combined oestrogen and progestogen HRT (now known as MHT, or menopause hormone therapy) before 60 or within a decade of menopause does not increase the risk of cardiovascular disease or stroke, slightly increases your risk of blood clots (by one extra case per 1000 for oral MHT, but not when using gels or patches) and does increase the risk of breast cancer, by approximately nine additional cases per 10,000 women.
Loading
“That’s a slightly higher risk than drinking a glass of wine a night, and less than drinking two glasses,” explains Ginni Mansberg. Being overweight or obese increases the risk more than taking MHT; women who exercise moderately for 2.5 hours a week lessen their risk more than they raise it by taking MHT. And if they take oestrogen-only MHT (following a hysterectomy), it may actually decrease heart disease and breast cancer risk. It doesn’t increase the risk of stroke, but does raise the risk of blood clots in the same way as combined MHT.
Oestrogen is also the gold-standard treatment for hot flushes (up to 98 per cent effective); it’s independently approved in Australia as a treatment for osteoporosis; it’s an effective treatment for genito-urinary issues like incontinence and dry vagina, and it can help what Ginni Mansberg calls “your lady bits, your skin, your sex drive, your weight distribution. All the fun stuff.”
“I think it’s connected to the fact that breast cancer is such a profound fear for women.”
You’d be forgiven for thinking at this point that every woman on earth should start taking oestrogen immediately. But you’d be wrong. Doctors don’t recommend it, even to women without risk factors, unless they have “bothersome” symptoms.
“And that means bothersome to you,” says Janet Michelmore, the CEO of the Jean Hailes Foundation, a national not-for-profit women’s health organisation named in honour of Michelmore’s mother, who started Australia’s first women’s health clinic, and one of the earliest menopause clinics in the world, in Melbourne in 1971.
“Menopause is a subjective experience: is it impacting your life?”
For the past two decades, Baber, Eden and other international experts have been trying to undo the damage of 2002. But in Australia today, only about 11 per cent of menopausal women take MHT. “It’s been a terrible 20 years,” says Eden. “Really the pits.”
“I think it’s connected to the fact that breast cancer is such a profound fear for women,” explains Baber. “And I don’t take that lightly – my first wife died of breast cancer. But the fact is, people are not all that aware of what’s going to kill them. Breast cancer is not the biggest killer of women. [It’s actually number five.] Dementia, including Alzheimer’s, kills more people than anything else, followed by heart disease.”
In almost all cases, of course, brain fog, forgetfulness and other cognitive challenges of menopause are only temporary. But they should not be underestimated. “I have a steady stream of articulate, intelligent women coming into my rooms,” says Eden. “And they say to me, ‘I’ve got dementia.’ What they’ve actually got is menopause.”
One of the places where women feel the impacts of menopause most is at work. Brain fog, hot flushes, incontinence and what one woman describes to me as “medieval-massacre periods” are rarely conducive to seamlessly awesome work performance.
“Menopause happens at exactly the time – late 40s, early 50s – when men are really starting to peak in their careers,” says Baber. “For women, it can be a real impediment.”
It’s no wonder AWU Queensland branch secretary Stacey Schinnerl believes work leave entitlements must be modernised. In an announcement last November, several national unions partnered with law firm Maurice Blackburn with the goal of enshrining menstrual and menopause leave alongside paid family and domestic violence leave in the Fair Work Act. Such a change, according to Schinnerl, would recognise “the health concerns women face, in contrast to men, who receive the same entitlements but experience none of those health hurdles”. Menstrual leave was granted in Spain in 2021; Japan, Indonesia, South Korea and Taiwan already have entitlements for forms of “reproductive leave”. “If women could choose,” said Schinnerl, “we would not experience this. We would like to opt out, but that’s not our reality.”
The only thing women can opt out of is work itself. In the same month as the union push, Australia’s peak superannuation body, the Australian Institute of Superannuation Trustees (AIST), released a report revealing that just over a quarter of Australian working women are retiring under the age of 55, four years earlier than the expected age of 59. Almost 50 per cent of these women, moreover, cite personal “sickness, injury or disability” as their reason for retiring. “Experienced middle-aged women [are] leaving the workforce at a time when they are at the peak of their experience and earning potential,” AIST CEO Eva Scheerlinck explained last year.
Loading
It’s unclear what role menopause plays in this decision, but recent British studies show that a quarter of menopausal women in the UK experience such debilitating symptoms, they’re forced into long-term absences or early retirement. The AIST wants the Office for Women to investigate the impacts of menopause here. “This is a great time for the work to be done,” says Scheerlinck now, “because women retire with 40 per cent less superannuation than men – and they live longer.”
Such investigations and entitlements are all very well in theory, of course. “But I worry that menopause leave will become a stick to beat women with,” says Elizabeth Farrell, a Victorian gynaecologist and the medical director (and co-founder) of Jean Hailes. “I hate to say it, but some employers will use it as an excuse not to employ women, and to not promote them.”
“Experienced middle-aged women [are] leaving the workforce at a time when they are at the peak of their experience and earning potential.”
A few days after the Christmas pudding afternoon, I was at a drinks party, talking to a friend – funny, competent, articulate – who’s a senior partner at a large Sydney accounting firm. She told me about her recent annual partner health check, which costs her employer a significant amount and lasts more than an hour. She’s in her late 40s, but at no point – “not even in the mental-health wellness discussion” – was she asked a single question about menopause. She was bemused by this – but nonetheless baulks at the thought of discussing menopause in the workplace herself.
“There’s just no way,” she told me. “I mean, I would love to help the sisterhood. But I’ve spent the last 20 years basically convincing all the men I work with that I am a man. ‘It’s okay, I am not emotional, my needs and style are no different from yours.’ The thought of turning round and saying, ‘Actually I’m going through a whole lot of stuff and I do need different things right now’? It’s just impossible.”
Peta Murphy, federal member for Dunkley in Victoria, knows what it’s like to go through menopause in the workplace. She was 37 years old, working as a criminal barrister and hoping to get pregnant, when she was diagnosed with breast cancer in 2011. An intense three months of chemotherapy, and injections to try to protect her fertility, catapulted her into menopause. “I’d have these full-on hot flushes,” she recalls. “I was visiting my sister in Calgary and it was, like, minus 27 degrees, so I was wearing all the gear, and I remember being so hot and sweaty I had to take absolutely everything off.” Once her treatment finished she came out of menopause, and she and her husband tried, with no luck, to have children. At 43, she had a hysterectomy.
She was elected to Parliament for her south-east Melbourne seat in 2019. Two days after being sworn in to Parliament, and a fortnight before her maiden speech, she discovered her cancer had returned. Since then, along with all the other horrors of cancer treatment, she’s had to deal with menopause all over again.

Federal MP Peta Murphy: “We need to be talking about menopause in the same way we’re talking about periods,” she says, “and taking action in the same way.”Credit:Alex Ellinghausen
This time around “feels the same, really: as if my thermostat is broken. I’d be sitting in the chamber during question time and realise my face was sweating; my shirt was wet under my suit. It’s no different from what every other working woman goes through, but it becomes really hard to concentrate. You’re thinking, ‘Can I take my jacket off? Is anyone noticing that my face is red? Can I go outside for a little while?’ It’s not like a coughing fit. You can’t say, ‘Sorry everyone, can you just give me 30 seconds and I’ll be fine.’ You should be able to, but you can’t.”
The other problem for Murphy is that because her cancer is hormone-receptor positive, she can’t take oestrogen. Instead, her doctors have prescribed a low-dose antidepressant to combat the hot flushes and night sweats. “It’s been amazing, and I’ve told lots of women about it, because nobody seems to know.”
“It’s not like a coughing fit. You can’t say, ‘Sorry everyone, can you just give me 30 seconds and I’ll be fine.’ You should be able to, but you can’t.”
There are in fact, several effective prescription alternatives to MHT. Diet, exercise, cognitive behavioural therapy and – oddly – hypnosis have also been scientifically proven to help. There are also myriad alternative treatments. Some of these are harmless, some appear to work for some people, and many are yet to be subject to rigorous scientific study. Some, however, worry medicos. Dr Krishna Ghosh is a Sydney GP who sees up to three women a day about menopause. “There are some women who are strongly against taking prescription medication, which is fair enough,” she says.
“But they’re often spending really significant amounts of money on alternatives, especially things like [compounded] bioidentical hormones.” Marketed as natural alternatives to pharmaceutical-grade, TGA-approved therapies, these formulations have generally not been tested for safety or effectiveness. They’ve also been associated with cases of endometrial cancer. The Australasian Menopause Society “does not recommend the use of compounded bioidentical hormone therapy in any form.”
“It’s important for women to know that there are good, safe medical treatments that can mitigate the symptoms for you,” says Murphy. “Your transition to the next phase of your life can be made so much easier: you don’t have to suffer.
Loading
“I do think things are changing,” she adds. “And that’s because there are more women in parliament, more women in research, more women in journalism. Victoria has just announced free sanitary products in schools and public toilets. We need to be talking about menopause in the same way we’re talking about periods, and taking action in the same way.”
At the end of our Christmas pudding day, my friend and I sat on the deck as the sun set. What’s life like after menopause, I asked her. “Oh, I don’t know,” she said. “I’m not sure I’m really through it – I still get the odd hot flush. But hopefully it’s like Kristin Scott Thomas in Fleabag, where she says that thing … now I can’t remember it. That’s bloody menopause for you.”
What Scott-Thomas says, in one of the great monologues of the Emmy Award-winning series, is: “Yes. Your entire pelvic floor crumbles and you get f—ing hot, and no one cares. But then you’re free. No longer a slave, no longer a machine with parts.” Which reminds me, in turn, of an interviewee in a New York Times documentary about menopause, who said that being post-menopausal is “like being 10 again. Before the hormone changes of puberty – back when I just felt like, ‘This is me. I know who I am.’ It’s as if oestrogen was this weird drug you were on, and now you’re coming out the other side, and you’re like, ‘Wow. That was a weird trip.’ ”
All in all, it’s just another thing women have to deal with, says my friend. “But, you know, you can’t spend your whole life worrying about it. Just remember, during the pandemic, we all learnt to say ‘epidemiologist’. We can talk about menopause, too.”
We certainly can – because after all, as Baber puts it: “We’re really talking about midlife women’s health. And that’s half our population, and around a third of their lives. So it’s a conversation we have to have.”
To read more from Good Weekend magazine, visit our page at The Sydney Morning Herald, The Age and Brisbane Times.
Stay connected with us on social media platform for instant update click here to join our Twitter, & Facebook
We are now on Telegram. Click here to join our channel (@TechiUpdate) and stay updated with the latest Technology headlines.
For all the latest Life Style News Click Here
For the latest news and updates, follow us on Google News.